Nursing Professional Practice Model
The Professional Practice Model (PPM) at Memorial Hospital is a common way of understanding and describing nursing regardless of practice setting.
The PPM is based on Jean Watson’s, PhD, RN, AHN-BC, FAAN, LL (AAN) Theory of Human Caring, which describes the profound nature of caring and specific healing practices. The construct of caring as described by Dr. Watson’s and other similar nurse theorists is the essence of nursing practice and has been operationalized into the transformational model, Relationship-Based Care® (RBC), which provides the conceptual framework for care delivery. The current nursing PPM was developed in 2010 and has been evaluated and revised since its conception.
To weave RBC into the fabric of Memorial, the organization has established the expectation that all employees attend a three-day retreat, Reigniting the Spirit of Caring (RSC). The organization has provided RSC since 2010. Trained facilitators lead 8–10 RSC retreats annually.
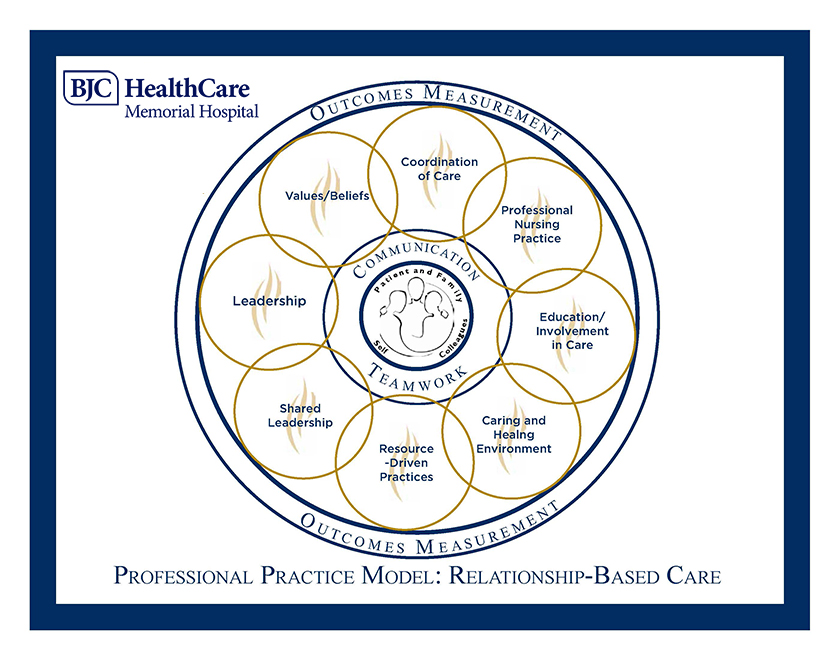
The PPM is a blueprint for nursing at Memorial, depicting through its schematic, how nurses at Memorial Hospital–Belleville and Memorial Hospital–Shiloh practice, collaborate, and develop professionally to provide the highest quality of care to the patients they serve.
The PPM schematic illustrates the three defining relationships of RBC in the center of the model, which serve as the foundation for the PPM. Caring practices are activities that are responsive to the individual patient and family’s unique needs and create a compassionate, therapeutic environment. The core relationships are surrounded by two essential components of RBC: communication and teamwork, which are integral to every successful relationship.
The three relationships are:
- Relationship with self
- Awareness
- Balance
- Self-care: A fundamental requirement for quality care
- Relationship with colleagues:
- Mutual respect
- Trust
- Open, honest communication
- Consistent, visible support
- Relationship with patients and families:
- Patient and family are the central focus of our work
- Caring for mind, body, and spirit
- Learning what is most important to the patient and family
- Engaging the patient in all aspects of their care
Additionally, Memorial has defined eight supporting components of nursing practice that are intertwined, overlapping each other. The eight domains are surrounded by outcome measurements, which define the impact of nursing practice in a healthy work environment. These eight interwoven components (circles in the PPM schematic) strengthen the three relationships at the core of the PPM and are outlined below.
Leadership
RBC “calls forth the leader within each one of us.” It asserts that every nurse is a leader, whether leading from the bedside or from an executive role. This occurs when individuals take ownership for their work. Leadership development prepares nurses at all levels to assume professional roles in practice, leadership, education, and research. Caring and compassion are leader behaviors.
Values and beliefs
The culture of the organization is a collection of traditions, beliefs, values, and behaviors that comprise the context for how care is delivered.
Coordination of care
Coordination of care is an essential component of high quality, safe patient care.
- Coordinated care begins upon entry to Memorial and continues through discharge.
- The nurse responsible for the patient when the patient presents for care takes ownership for the patient’s safety and satisfaction.
- The responsible nurse is accountable for coordinating patient care and communicating the patient’s condition, priorities, and concerns during transfer of care.
- The responsible nurse communicates with interprofessional colleagues to coordinate care and meet patient-specific and family needs.
Professional nursing practice
Professional nursing practice is the cornerstone of care delivery and exists within a caring and therapeutic relationship between a nurse and patient.
- Continuity of the nurse and patient relationship is supported by the health care team through work schedules and assignments.
- The nurse has authority to delegate nursing activities to other caregivers of the interprofessional team consistent with the scope of practice defined in the Illinois Nurse Practice Act.
- The responsibility and accountability for professional growth and development are shared by the nurse and organization.
- The ANA Code of Ethics for Nurses and Scope and Standards of Nursing Practice are integrated.
Education and involvement in care
The nurse and patient are mutually responsible for determining the plan of care and outcomes. The nurse:
- Provides education and guidance that addresses healthy lifestyles, developmental needs, preventive self-care, and risk-reducing behaviors.
- Uses teaching methods appropriate to the situation and patient’s developmental level, learning needs, language preference, and culture.
- Provides educational resources to help patients understand diagnostic tests, diagnoses, medications, and follow-up required.
Caring and healing environment
Quality care attends to the whole person—mind, body, and spirit. The combination of therapeutic relationships and an environment that provides comfort and meets the patient and family’s physical needs promotes healing. It includes the following beliefs:
- Initiating and sustaining a healing environment creates the environment for healing.
- Care innovations and system design impact the therapeutic relationship between a nurse and patient.
- A caring and healing environment creates circumstances for patient-centered, relationship-based care.
Resource-driven practice
This component focuses on what resources are available and prioritization of what matters most to the patient and family to be a strong steward of resources.
- Clinical staff, managers, and supervisors share responsibility for resources to provide quality care.
- A new mindset encourages “resource-driven” thinking versus “needs-driven” thinking.
- Critical thinking, creative thinking, and reflection help transform ineffective ways of thinking and doing work.
- Resource allocation requires commitment of all staff including clinical nurses, managers, and nurse leaders.
- Continuity of care promotes increased productivity and patient safety.
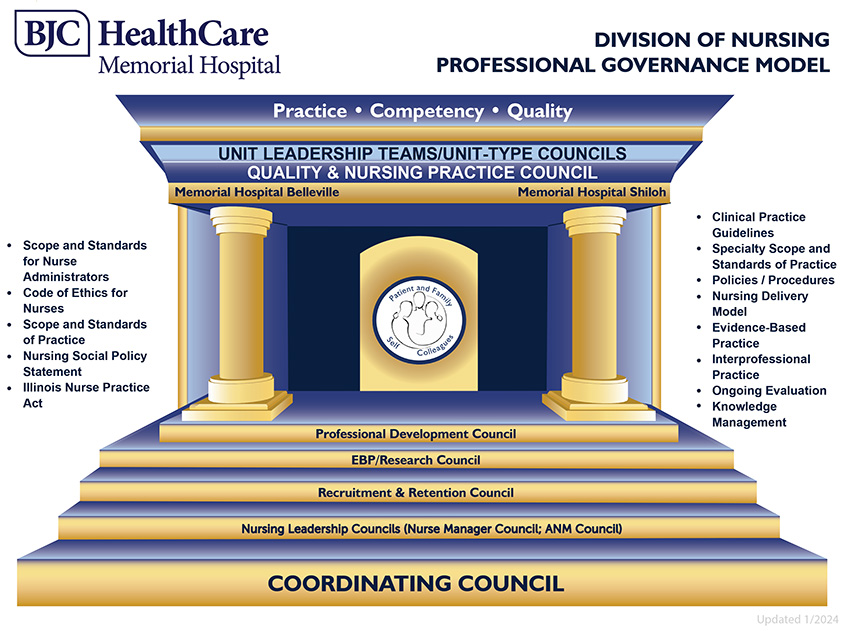
Nursing professional governance
Sharing leadership (professional governance) serves as the foundation for the shared decision-making between management and the clinical nurses, placing the authority, autonomy, and accountability for nursing practice at the bedside with clinical nurses.
Nursing’s professional governance model was developed in 2004 and has been revised and updated on an ongoing basis to meet the needs of the organization and the goals for the nursing services department.
- This model empowers all members to have a voice in decision-making.
- It empowers professional clinical nurses, nurse managers, and nurse leaders to contribute collectively to the decision-making process related to nursing practice, standards, and procedures. Shared leadership contributes to improved patient outcomes.
- Memorial’s nursing services department has five central governance councils and a coordinating council, which oversees the activities of the other councils.
- Each unit and service line has a unit leadership team (ULT) and unit-type council (UTC) whose role is to plan, implement, and continuously improve the practice, quality, and competency for their unit and service line patient population.